
1
1A. Visual Acuity in Refraction and Refractive Error
[1.] Visual Acuity
In V550, you learned how to take visual acuities as an entrance test. The rule of thumb was that a person could read a line of acuity if they read MORE than half the letters. Why is this the rule? Its because if they read more than half the letters, the statistically probability makes it near impossible they randomly guessed those letters. For simplicity sake, lets assume all 26 letters of the alphabet are used in a chart (they are not all used, more later.) Most rows of acuity have 5 letters in them. What is the probability of randomly guessing correctly 3 out of those 5 letters?
26 X 26 X 26 or 26^3 = 1 in 17,576
In this example, there is a 1 in over 17,000 chance that you could randomly guess 3 correct letters. If a patient can read 3 out of 5 letters, it is virtually impossible for them not to be able to see that line of acuity.
Blurry, but Readable
Examine the top row of all three charts below. In all three, the top row letters are readable and someone seeing like this would get MORE than half of those letters. We would also all agree that we can perceive blur in the letters for the last two. It is for this reason, we DO NOT ask the patient “can you read the letters?” because many patients will say those letters are blurry and say they cannot read them. We make them read the letters. This is also true during refraction. Make the patient read the letters.
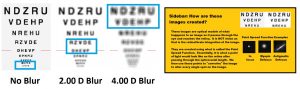 The blue boxes on each chart show the line/lines where people would read approximately more than half the letters. The image below shows a blown up image of the letters around the persons acuity. As a patient reaches their threshold, the patient begins to guess (sometimes an educated guess) to the point where they miss more than half the letters. In the example below, near threshold, some letters are still very distinct, some are unreadable, and some look offer the patient a small range of options (in the example below, O, G, and D look very similar.)
The blue boxes on each chart show the line/lines where people would read approximately more than half the letters. The image below shows a blown up image of the letters around the persons acuity. As a patient reaches their threshold, the patient begins to guess (sometimes an educated guess) to the point where they miss more than half the letters. In the example below, near threshold, some letters are still very distinct, some are unreadable, and some look offer the patient a small range of options (in the example below, O, G, and D look very similar.)
Rule #4: Always measure acuities, whether as an entrance test or during refraction, never ask subjective opinion
[2.] Visual Acuity and Refractive Error
For resolution of fine points, the visual system requires two things, 1. good optics and 2. appropriately spaced detectors (retina). Visual acuity can bet limited by either of these two. For the smallest point to be detected or the finest detail to be resolved, requires a good optical system and appropriately spaced detectors. Visual acuity will be limited by one of these.
Below is a visual acuity chart as a hypothetically perfect emmetropic patient without accommodation. This is what they would see as we put lenses in 0.50 D steps in front of their eye. At 0.00 diopters, the acuity chart looks the best. As blur is added, we begin to lose lines of acuity, and by the time we reach 3-4.00 diopters of blur, nothing can be read. In a situation WITHOUT ACCOMMODATION, this provides a fine endpoint that reaches the patient’s best acuity. This ideal situation only really exists in patients over the age of 55 (and is actually harder due to increased depth of focus).
Emmetropes Without Accommodation
Emmetropes With Accommodation
With accommodation, emmetropes can clear MINUS powered lenses up to their maximum accommodative range. In the example below, the patient can accommodate up to 2.50-3.00 diopters, so the acuity remains clear throughout as MINUS lenses are added. When PLUS lenses are added, no patients can clear (because we cannot negatively accommodate.) This is the reason we use PLUS lenses to control accommodation during the refraction testing.
Myopes With and Without Accommodation
Just like above, there is a critical lens where VA is maximized in myopes. The only difference is that the lens that maximizes acuity is more minus. Just like above though, myopes with accommodation can clear their vision as more minus power is added past the first best acuity. They will not see any BETTER, but it remains the same acuity. This event is called OVER MINUSING and should be avoided during the subjective refraction portion of the exam. We may choose to prescribe more minus during the prescribing step (typically due to habitual wear), but that is done at the end of refraction.
Hyperopes With and Without Accommodation
Hyperopia is a different ballgame, where the presence or absence of accommodation matters enormously for how the patient sees without correction. Let’s look at the example below of a +2.00 diopter hyperope with and without accommodation. WITH accommodation, the patient sees 20/20 at distance and may still see 20/20 at near depending upon the amount of accommodation they have. A patient WITHOUT accommodation can not see this well. They see 20/80 at distance and even worse at near. Again, in this example, the refractive error is the same, but the presence of accommodation drastically changes the acuities.
What happens during accommodation in a hyperope? The lens increases its curvature, thereby adding plus power to the lens. Unaccommodated eyes have the focal position BEHIND the retina. When the eye accommodates, this added plus power moves the focal position onto the retina, thereby allowing for 20/20 (or 20/15) vision.
[3.] MPMVA (Most Plus to Maximize Visual Acuity)
Most Plus to Most Visual Acuity (MPMVA) is the critical rule all optometrist live by when determining the end point for checking spherical refractive error (Myopia or Hyperopia). Essentially, it means what is the most plus powered lens that gives the best VA. Let’s use our hyperope with accommodation as an example below. There is a range of lenses that give 20/20 vision from +2.00 to -0.50 diopters. The rule is the MOST plus lens that gives the best acuity, so +2.00 D is the MPMVA. Sometimes the “V” is left off resulting in the acronym MPMA instead, which is fine.
[4.] Visual Acuity and Age
Acuity at birth begins at approximately 20/200, and approaches 20/20 within 3 years of life. This ignores refractive error for the moment, and just takes into account acuity with ideal optics. This is largely due to the lack of foveal development at birth and influx/packing of cone photoreceptors over the first three years to develop the fovea. By teenage years, 50% of the population can see 20/15 and is maintained until the 5th decade of life when cataracts begin to set in.
1B. Visual Acuity in Refraction and Refractive
Error
[1.] Why use Visual acuity to predict Refractive Error
Below is the isoacuity chart used in V550, updated with modern graphics to make it easier to understand. Even in this new format, it is a complex chart. The chart is colored in a heat map, with hotter/redder colors being worse acuity and cooler/bluer colors being better acuity.
Let’s look at the section around +/- 1.00 diopter in any direction below. This is the section the chart that is most useful for clinical practice. 90-95% of your patients will enter in this area. A smart person in the would look around the classroom/lab and see there are lots of high myopes in the room, so why is this section the most important? Because most patients enter WITH correction on, so their acuity is only reduced by a few lines.
Imagine two patients, one is an emmetrope and the other is a -6.00 D myope. Both have the same complaint of distance blur and both see 20/40 at distance, near is 20/20. In both situations, the CHANGE in refractive error is -0.75 D. for the first patient’s spectacle prescription will be -0.75 sph and the other -6.75, but the over the all change is the same. This is one of the important reasons to use VA to predict CHANGE in refractive error.
What we have shown you so far is acuities for patients with accommodation. Patients with hyperopia and accommodation can move the focal position, thereby reducing blur from both hyperopia and astigmatism. Patients without accommodation, the hyperopia effects vision as equally as myopia.
An arguably more important use of VAs is to predict refractive error is to guide you through refraction. This allows us to build a hypothesis of what the prescription/change in prescription is, which greatly reduces time spent refracting. As mentioned in other modules, there are literally thousands of possible lens combinations and to test them all would be silly. Predicting the refraction gives you a hypothesis to test and will limit the possibilities in most conditions down to a 2-4 options.
Guiding Rule #1 of refraction and prescribing: Never start refracting without knowing where you expect to go.
[2.] How does VA predict the amount of refractive error or the change in refractive error
Using the patient’s age as a surrogate for amount of accommodation, the visual acuities and where VAs are reduced (distance, near or both,) you should be able to predict what a patient’s rx or change in rx is. See the table below for the amounts and locations. As a general rule, sphere power reduces VAs by 0.25 D per line and astigmatism reduces VAs by 0.50 D per line.
[3.] Examples
These next examples illustrate the effects of no accommodation and limitations in predicting refraction from acuities in general.
These final examples are showing changes in refraction.