
83 Lifespan changes
Learning Objectives
After reading this section you should be able to-
- Compare and contrast female and male physiological sexual responses.
- Define menopause and describe the physiological changes associated with menopause.
- Compare and contrast menopause with andropause.
- Describe examples of how birth control methods disrupt normal reproductive function.
The following chapter will discuss the physiology of arousal and orgasm. Arousal includes the physiology of erection and increased lubrication production due to a combination of mental and physical stimuli. Orgasm typically includes the release of ejaculate and involuntary muscle contractions accompanied by feelings of euphoria. Immediately following orgasm there is resolution of vasocongestion in erectile tissue followed by feelings of contentment and relaxation.
Arousal
The physiological process of arousal can begin due to sexual thoughts or from physical stimulation. Mostly commonly, the combination of mental and physical input together – synapsing with the sacral nerves roots – leads to reflexive patterns of physiologic arousal. Due to the reflexive nature of the response, positive mental stimulation is it not a requirement for physical signs of arousal to occur. Also, in the case of spinal cord injury, the location of the injury relative to the sacral nerve roots will dictate whether input from the brain, or from physical stimulation, will lead to physical signs of arousal. Sexual sensations are typically most intense due to physical stimulation of the glans of the clitoris or penis, although arousal can also occur due to stimulation of the nipples, all portions of the clitoris and penis, the vulva and perineal region, prostate, urethra, bladder, anal epithelium, scrotum, testes and vas deferens. Efferent and afferent signals related to sexual arousal travel along many nerves including the pudendal, pelvic splanchnic, hypogastric, vagus, ilioinguinal, posterior femoral cutaneous and genital branch of the genitofemoral nerve.
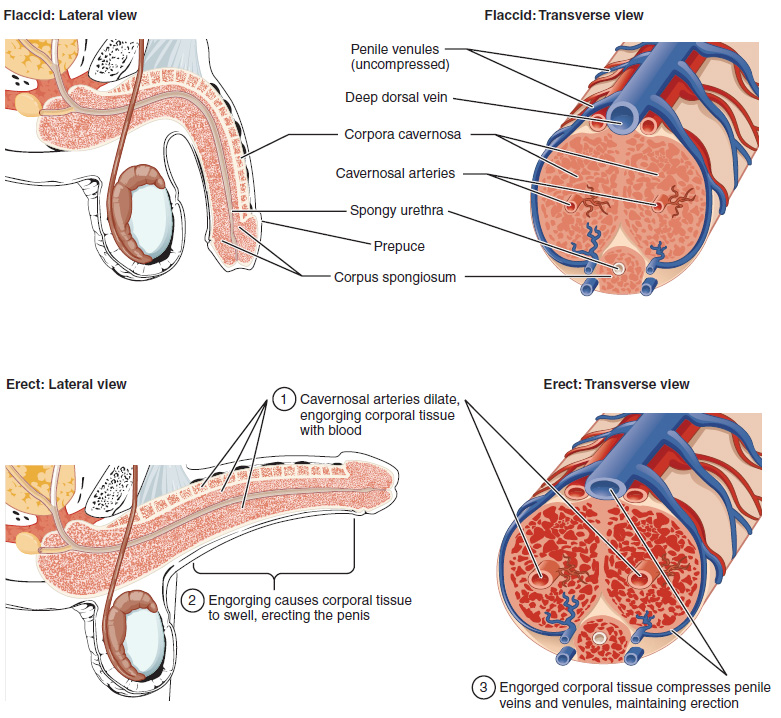
The clitoris, the bulbs of the vestibule and the penis are erectile tissues. Erections are the result of vasocongestion, or engorgement of the tissues because of more arterial blood flowing into the erectile structure than is leaving in the veins. During sexual arousal, nitric oxide (NO) is released from parasympathetic nerve endings near blood vessels within the corpora cavernosa and spongiosum. Release of NO activates a signaling pathway that results in relaxation of the smooth muscles that surround the arteries, causing them to dilate. This dilation increases the amount of blood that can enter the erectile structures and induces the endothelial cells in the arterial walls to also secrete NO and perpetuate the vasodilation. The rapid increase in blood volume fills the erectile chambers, and the increased pressure of the filled chambers compresses the thin-walled venules, preventing venous drainage. The result of this increased blood flow to the erectile structures, and reduced blood returning from the structure, is called erection.
Parasympathetic impulses during arousal cause the secretion of mucus from the greater vestibular glands into the vestibule of the vulva via a pair of ducts found lateral to the vaginal opening. Instead of mucus, the capillaries of the vaginal walls secrete serous fluid as vaginal lubrication. Arousal also causes the bulbourethral glands of the penis to release mucus into the urethra – which is referred to as pre-ejaculate or pre-cum. This release of mucus removes urine and old sperm from the urethra and provides lubrication for semen during ejaculation. If there has been a recent ejaculation, and the pre-ejaculate may have viable sperm in it.
Orgasm
When the mental and/or physical stimuli have reached a necessary threshold, the spinal cord emits sympathetic impulses that lead to orgasm. Orgasm was defined by sex researcher Alfred Kinsey in 1953 as “The expulsive discharge of neuromuscular tensions at the peak of sexual response.” Others describe orgasm as climax or an altered state of consciousness. Neuroimaging studies have observed that during orgasm the prefrontal lobe and portions of the temporal lobe have decreased activity, while brain regions such as the nucleus accumbens (award center), amygdala (emotional center), hippocampus (memory), cerebellum (coordinated muscle tension) and hypothalamus (release of oxytocin) have an increased level of activity.
Overlaying the crus (legs) of the clitoris and penis are the ischiocavernosus muscles, while the bulbs of the vestibule and the bulb of the penis are covered by the bulbospongiosum. During orgasm, these involuntary muscles undergo rhythmic contraction, as do other perineal and pelvic and trunk muscles. There is evidence to suggest that the cervical canal dilates during orgasm, and that uterine motility is increased. Ejaculation through the urethra has the potential to occur in all individuals due to release of fluid from the prostate or female prostate. In some cases, ejaculation is retrograde, meaning that the fluid moves towards the bladder and may go undetected. The anatomical length of the urethra can influence the likelihood of retrograde ejaculation, and is more common in individuals with a short, rather than long, urethra. Contraction of the vas deferens and ampulla causes expulsion of sperm into the urethra, and contraction of the seminal vesicle and prostate add fluids to fill the urethral and produce reflective ejaculation of semen. The refractory period necessary between one orgasm and the next is highly variable and explains why some individuals can experience multiple orgasms, while others cannot.
The health benefits of orgasm have been investigated by some, and the results suggest that regular orgasm can improve sleep, decrease stress, decrease chronic pain, and decrease risk of incontinence and even mortality during aging. If sex will involve vaginal penetration, orgasms prior to penetration may be especially important to ensure that vaginal lubrication levels are sufficient to decrease the chance of laceration of the vaginal walls (vaginal laceration increases transmission of disease). There is also evidence to suggest that orgasms help decrease the chance of urinary tract infection following sexual activity due to the flushing of the urethra during ejaculation.
Resolution
Within 1-2 minutes following orgasm, the resolution of the vasocongestion in the erectile tissues occurs (assuming cessation of the physical and/or mental stimuli, or inability for multiple orgasm due to the absolute refractory period). The smooth muscle of the artery walls is no longer relaxed due to NO release, and returns to its baseline vasomotor tone. This decreases the blood flow to the erectile tissues, equalizing the volume of blood entering and leaving the erectile chambers, and returning the structures to their non-erect size and shape. The hormones released upon orgasm, such as oxytocin, lead to the feelings of contentment and well being.
Menopause and andropause
A well-known example of the aging process affecting an endocrine gland is menopause and the decline of ovarian function. With increasing age, the ovaries decrease in both size and weight and become progressively less sensitive to gonadotropins. This gradually causes a decrease in estrogen and progesterone levels, leading to menopause and the inability to reproduce. Low levels of estrogens and progesterone are also associated with some disease states, such as osteoporosis, atherosclerosis, and hyperlipidemia, or abnormal blood lipid levels.
Testosterone levels also decline with age, a condition called andropause (or viropause); however, this decline is much less dramatic than the decline of estrogens in women, and much more gradual, rarely affecting sperm production until very old age. Although this means that males maintain their ability to father children for decades longer than females, the quantity, quality, and motility of their sperm is often reduced.
Birth Control
Moving beyond the physiological changes associated with menopause and andropause, it’s essential to discuss contraceptive methods. The evolution of reproductive healthcare has ushered in innovative solutions designed to enhance convenience, effectiveness, and individual preferences.
Birth control pills take advantage of the negative feedback system that regulates the ovarian and menstrual cycles to stop ovulation and prevent pregnancy. Typically they work by providing a constant level of both estrogen and progesterone, which negatively feeds back onto the hypothalamus and pituitary, thus preventing the release of FSH and LH. Without FSH, the follicles do not mature, and without the LH surge, ovulation does not occur. Although the estrogen in birth control pills does stimulate some thickening of the endometrial wall, it is reduced compared with a normal cycle and is less likely to support implantation.
Some birth control pills contain 21 active pills containing hormones, and 7 inactive pills (placebos). The decline in hormones during the week that the woman takes the placebo pills triggers menses, although it is typically lighter than a normal menstrual flow because of the reduced endometrial thickening. Newer types of birth control pills have been developed that deliver low-dose estrogens and progesterone for the entire cycle (these are meant to be taken 365 days a year), and menses never occurs. While some women prefer to have the proof of a lack of pregnancy that a monthly period provides, menstruation every 28 days is not required for health reasons, and there are no reported adverse effects of not having a menstrual period in an otherwise healthy individual.
Because birth control pills function by providing constant estrogen and progesterone levels and disrupting negative feedback, skipping even just one or two pills at certain points of the cycle (or even being several hours late taking the pill) can lead to an increase in FSH and LH and result in ovulation. It is important, therefore, that the woman follow the directions on the birth control pill package to successfully prevent pregnancy.
In recent years, advancements in reproductive health have led to the development of innovative contraceptive methods that offer increased convenience, effectiveness, and flexibility compared to traditional options. These modern approaches aim to address the diverse needs and preferences of individuals, contributing to more personalized and accessible family planning.
One notable advancement is the introduction of hormonal patches, which provide an alternative to daily oral contraceptives. These patches, typically worn on the skin, release a continuous, low dose of hormones such as estrogen and progestin. The convenience of a once-weekly application offers a user-friendly option, reducing the chances of missed doses and improving overall adherence.
Intrauterine devices (IUDs) have also gained popularity as a highly effective and long-term contraceptive solution. These small, T-shaped devices are inserted into the uterus, where they can prevent pregnancy for several years. IUDs come in hormonal and non-hormonal varieties, catering to individual preferences and medical considerations. The non-hormonal IUD primarily utilizes copper, providing an effective barrier to sperm without hormonal side effects.
Implants represent another cutting-edge contraceptive method. These small, matchstick-sized devices are inserted under the skin of the upper arm, where they continuously release progestin to inhibit ovulation and thicken cervical mucus. Implants offer extended contraceptive protection, with some lasting up to three years, eliminating the need for daily or monthly attention.
Adapted from Anatomy & Physiology by Lindsay M. Biga et al, shared under a Creative Commons Attribution-ShareAlike 4.0 International License, chapter 27.
